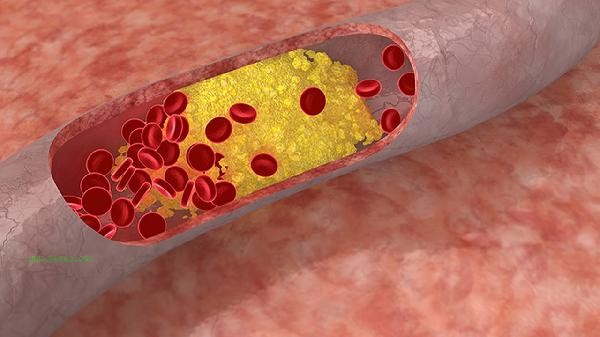
High average red blood cell concentration may be related to factors such as dehydration, long-term smoking, chronic obstructive pulmonary disease, polycythemia vera, congenital heart disease, etc. Further evaluation is required based on specific examination results and clinical manifestations.
1. Dehydration
Loss of body fluids leading to blood concentration is a common physiological cause. Failure to replenish water in a timely manner after intense exercise, long-term diarrhea, or high fever and sweating can all cause temporary elevation of indicators. By supplementing electrolyte solution and increasing water intake, indicators can usually return to normal. Daily water intake should be maintained at 1500-2000 milliliters to avoid prolonged exposure to high temperatures.
2. Long term smoking
Carbon monoxide in tobacco can combine with hemoglobin to form carboxyhemoglobin, leading to tissue hypoxia and stimulating compensatory bone marrow proliferation. Smokers often have this indicator consistently higher than normal, which may cause symptoms such as dizziness and lip cyanosis. After quitting smoking, relevant indicators can gradually improve 3-6 months later, and lung function assessment may be necessary if necessary.
3. Chronic obstructive pulmonary disease
Chronic hypoxia can stimulate the secretion of erythropoietin by the kidneys, leading to secondary erythrocytosis. Patients often have symptoms such as coughing and shortness of breath after physical activity, and arterial blood gas analysis shows a decrease in blood oxygen pressure. Low flow oxygen therapy, bronchodilators, and other treatments are needed to improve ventilation function. In severe cases, blood dilution therapy is required.
4. Polycythemia vera
Bone marrow proliferative tumors lead to autonomous proliferation of red blood cells, which may be accompanied by an increase in platelets and white blood cells. Typical symptoms include skin and mucous membrane congestion, headache, and splenomegaly, and JAK2 gene testing can assist in diagnosis. The treatment requires the use of bloodletting therapy combined with cell suppressive drugs such as hydroxyurea tablets, and regular monitoring of thrombus risk.
5. Congenital heart disease
Cyantic congenital heart disease with right to left shunt can cause chronic hypoxemia, commonly seen in diseases such as Tetralogy of Fallot. Children with clubbing fingers and developmental delay are often present, and cardiac ultrasound can provide a clear diagnosis. Surgical correction or interventional treatment should be selected according to the condition, and long-term follow-up of blood routine changes is required after surgery. When abnormal indicators are found, blood routine should be rechecked and examinations such as reticulocyte count and iron metabolism should be completed. Avoid high-altitude travel and vigorous exercise in daily life, and control the daily salt intake to below 5 grams. Patients with polycythemia vera require prophylactic use of aspirin enteric coated tablets for anticoagulation and regular blood rheology testing. All patients should be monitored for dynamic changes in blood routine every 3-6 months. If there are symptoms of blood clots such as blurred vision or limb numbness, immediate medical attention should be sought.








Comments (0)
Leave a Comment
No comments yet
Be the first to share your thoughts!